How do UBC’s bureaucratic and institutional structures perpetuate ableist assumptions such as burden discourse?
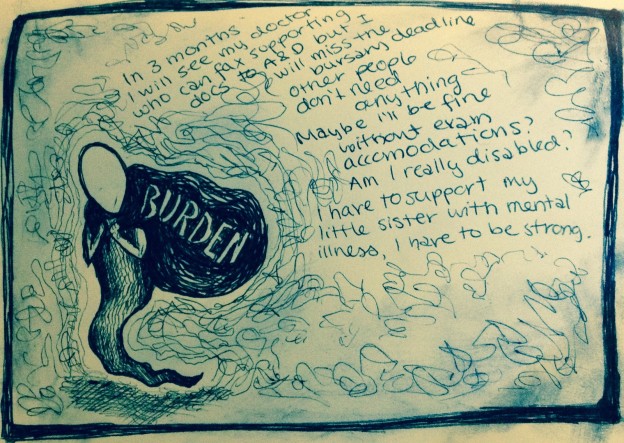
Burden discourse is when disabled bodies don’t feel entitled to ask for support. This can be due to language use, interpersonal interactions, and/or structures in the institution, which is what this article will focus on.
It is critical to look closely at how bureaucratic architecture and institutional structures influence and shape our experience at UBC as disabled students and allies. Not only is this necessary to better understand and identify how the institution affects our bodies, but it is imperative to analyze how UBC views, understands, and enforces the role of disabled bodies in the institution.
Although UBC’s primary source of disability support, Access and Diversity (A&D), provides necessary guidance, it also has much room for improvement. For instance, during my first visit to A&D, I was asked what accommodations I need to have “success” at UBC. At the time, I asked for exam accommodations because it was the only support they had mentioned was available. In my following years at UBC I’ve learnt that there are many more resources available, such as bursaries, scholarships, hired note-takers, and computer programs. Because we live in an ableist society (ableism is the “discrimination or prejudice against individuals with disabilities”, see this Social Justice Synonyms article for more information on ableism), I did not know that I was entitled to ask for further resources. I was not aware of the huge range of support available and that I in fact deserved and was well entitled to these services.
Further, the focus on success itself is also fraught: many notions of success within academia are ableist. Ableism in universities is institutionalized through structures and organization, such as the expectation of taking at least 5 classes a term and 27 credits a year in order to qualify for awards and scholarships. As it so often does, ableism here becomes tied with classism, as financial aid is awarded to those with the ability to match the expected workload. Although with permanent disability status through A&D you are eligible for grants through the government, UBC offers a very limited amount of financial support to its disabled students in comparison. “Success at UBC,” therefore, is not only an individual’s capacity to learn and study, but also constructed from a complex network of power relations.
These are major issues in terms of burden politics.
Not feeling entitled to support (or feeling like a ‘burden’) is an internalized manifestation of ableism, and therefore A&D, and any other form of disability support on campus, must set a precedent of undoing ableist conditioning to fully support disabled students and allies. This includes educating students that receiving disability support is not supplementary to an education but a right, that ableism is directly linked to capitalism and production politics, and that ability is not a percentage scale but rather a deeply personal and intimate relationship to the world around us. Although working within institutional ableist frameworks is often necessary for social organizations such as A&D to survive, failing to challenge ableism at every intersection is a way of fulfilling institutional policies while simultaneously creating a form of accessibility that is not centred on disabled students. By setting an example of actively working to undo ableist barriers, both internalized and structured by the institution, A&D and others would have the opportunity not only to shift institutional structures and non-disabled folks’ perspectives, but also allow disabled students to begin to imagine an institution that dismantles burden politics.
Disability support is generally based on the disabled person defining their own needs and asking for what is necessary to survive, but asking for help in an institution such as UBC is very complex. For instance, in order to be accepted as an Access & Diversity student, you must have supporting documentation from a medical professional. The university sees this as a means of ensuring the legitimacy of students’ needs, or in other words, that the disabled student is ‘disabled enough’ to be supported financially by the university. Not only does this perpetuate ableist assumptions that people exaggerate their disability or ongoing medical conditions to take advantage of resources (which extends beyond the university to Persons With Disabilities benefits and welfare), but it creates a barrier and binary of student ability and needs. With limited resources, this is perhaps necessary for Access and Diversity, but if the university prioritized addressing ableism, then these resources could be made available to students of all ability and needs, no matter their supporting documentation.
Further, making supporting documentation a basis of disability support heightens social barriers to access. Sexism, racism, heteronormativity and classism are prevalent in doctor–patient interactions. Many medical diagnoses are heavily influenced by a doctor’s perception of their patient, which allows for these social dynamics to come into play. When it comes to invisible illness, for instance, diagnosis is based on both tests and the patient’s narrative of their experience with illness. The doctor plays an active role in listening to the patient and while functioning within the white-dominant patriarchal framework of the Western medical system, there is most certainly the risk of prejudice influencing assumptions the doctor makes about the patient’s experience. Moreover, many invisible illnesses are difficult to diagnose and can therefore can take many years to define, which is even more challenging since an average waitlist in Canada for a specialist is over two months, contributing to the problem and inhibiting support for all the years prior to diagnosis.
Another example is sexism. Defining women’s complaints as hysteria has a long history in the Western medical institution, and although hysteria is no longer present in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), sexist assumptions that women’s complaints are exaggerated and not valid are still very much alive in patient-doctor interactions.
Further, racism has often justified manipulative and downright dangerous medical practices, including various experiments on Indigenous communities in Canada/Turtle island. This is but one example of how the Western medical system has been and continues to be a tool in Indigenous genocide and colonial violence. Although this history may not be overtly present in every doctor-patient interaction, the power dynamic of colonial doctor/Indigenous patient influences medical spaces.
Disability is inextricably linked to race on both a local and global scale. Intergenerational trauma as a result of colonialism and genocide disables Indigenous racialized bodies. Environmental degradation, political crisis and diaspora disables racialized bodies. Acknowledgement of these forces has to be at the forefront of disability support on every level, especially in a university that exists on xʷməθkʷəy̓əm (Musqueam) land and hosts thousands of international students. An institution that truly understands disability must actively work to support students that are living with the effects of such forces in their families, homes and bodies.
Because the process of getting support as a disabled person or an ally (of ‘coming-out’, of identifying oneself and asking for support) is met by oppressive barriers, such as sexism, racism, and ableism, and enforced by bureaucratic paperwork, the institution makes it very clear that you must prove that you are a ‘worthy burden’ to the economy of the establishment.
A burden is “something that is exacting, oppressive, or difficult to bear,” which is how I would define the challenges of navigating institutional burden politics at UBC. You are not a burden. The exacting, oppressive and difficult-to-bear burden is the labyrinth of paperwork, social barriers and ableist framework that we have to wade our way through to claim space.
Mental health resources on campus
First Nations House of Learning: 604.822.8940 First Nations House of Learning (counselling for Aboriginal students) 1985 West Mall Vancouver, BC Canada V6T 1Z2
Counselling Services, Student Services Brock Hall: 604.822.3811 Fax: 604.822.4957 Brock Hall 1874 East Mall Room 1040 Vancouver, BC Canada V6T 1Z1
Sexual Assault Support Centre, Emotional Support and Intervention: 604.822.3475. Nest 3127 6133 University Boulevard Vancouver, BC Canada V6T 1Z12



